TABLE OF CONTENTS
Uterine Inertia in Animals: Causes, Types, Clinical Signs & Treatment
Uterine inertia is a common cause of dystocia in animals, especially in dogs, cows, and sows. This article explains the types, clinical signs, causes, and treatment options to help veterinary professionals manage this condition effectively.
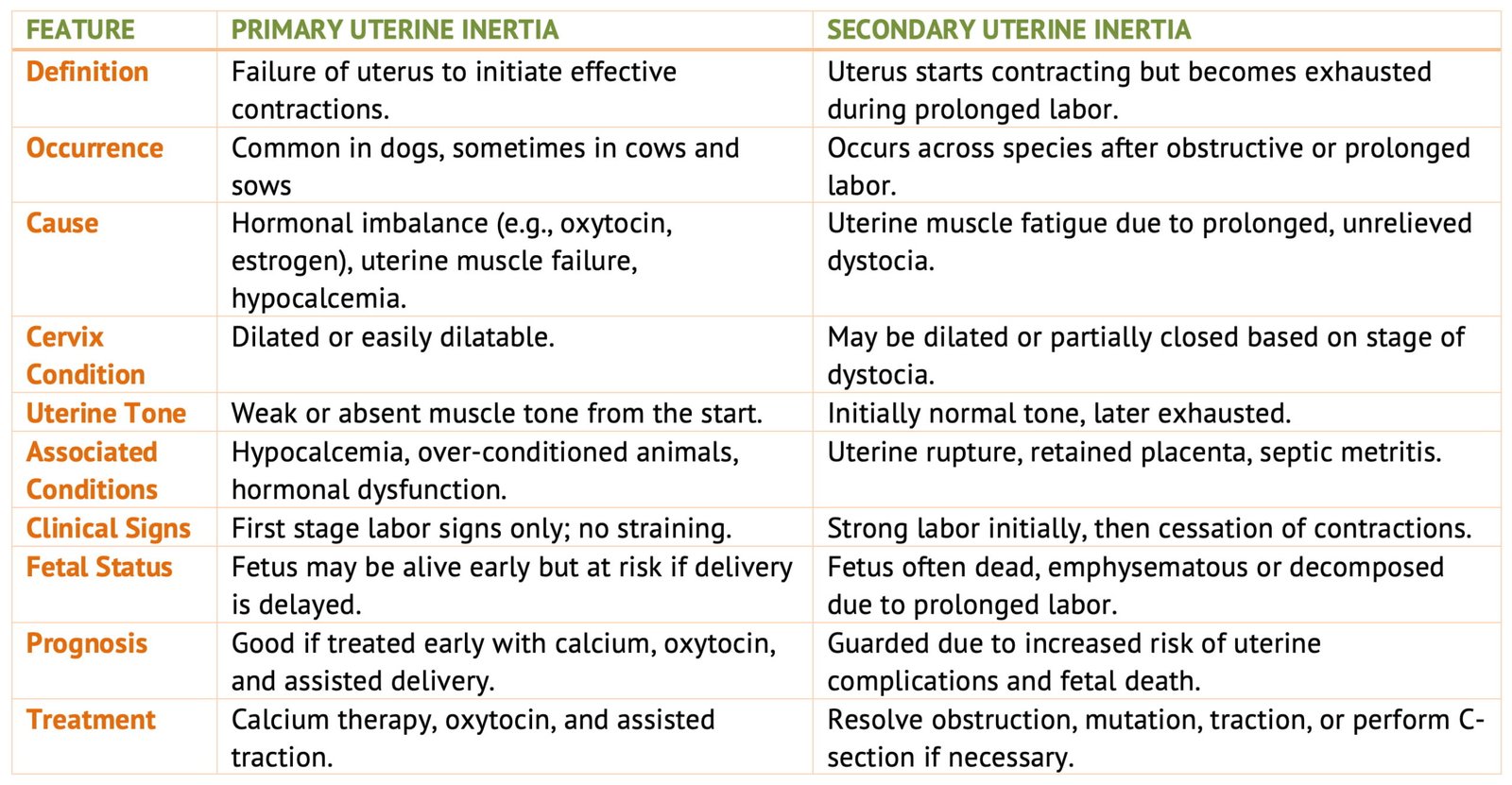
Uterine inertia is defined as the lack of normal physiologic uterine contractions during or after parturition. Two types of uterine inertia are recognized, primary and secondary.
Primary Uterine Inertia
Primary uterine inertia is seen most often in the dog, occasionally in the cow and sow, and rarely in the mare or ewe.
The failure of the uterine muscles to contract normally at parturition may be due to a primary failure of the muscles to respond to hormonal stimuli, possibly due to disease of the muscle; or it may result from an actual lack or failure of release of hormones, such as estrogens and possibly oxytocin, that initiate uterine contractions in normal muscles.
The most common cause is hypocalcemia.
The following conditions may be factors causing primary uterine inertia or a lack of uterine tone and feeble contractions at the time of parturition:
- It is observed more often in animals that are closely confined and hence lack exercise.
- It is more common in dairy than in beef cattle.
- Excessive fat may be a possible factor in dogs and other species.
- Certain brachycephalic breeds of dogs tend to develop uterine inertia despite the size of the litter. In dogs, it is observed more frequently in certain small breeds such as the Dachshund.
- Overstretching or overloading of the uterus in hydrops and twin pregnancy in cows, and a large number of fetuses in small dogs and sows, favour uterine inertia.
- It is observed more often in older dairy cows and dogs. It is frequently associated with debility or debilitating diseases.
- It may possibly be associated with disease or degeneration of the uterine wall due to uterine infections or secondary to peritonitis, as in traumatic peritonitis.
- It may be associated with an improper stimulus being applied to the posterior pituitary gland, a deficiency of that gland, or an inability of the uterine musculature to respond to the stimulation of oxytocin. Since the hormonal mechanisms of parturition are not completely understood, other hormonal imbalances may play a part in the production of primary uterine inertia.
Animals affected with primary uterine inertia are usually and obviously in the first stage of labor, as indicated by relaxation of the soft pelvic structures, marked mammary development, and discharge of mucus from the vulva.
The animals show no signs of distress and eat and drink almost normally, but the second stage of labor does not occur for 6 to 36 hours or longer, if at all. On examination, the cervix is usually relaxed and dilatable, but the fetus and fetal membranes are not being forced into the cervix or birth canal.
In some cases in cattle, the cervix fails to dilate normally due to a lack of hormonal stimulation or failure of the uterus to contract. In fact, failure of the cervix to dilate may be a manifestation of primary uterine inertia.
One or both fetal membranes may have ruptured. There is no abnormality in the presentation, position, or posture of the fetus. The uterus apparently fails to contract and push the fetus through the cervix and into the birth canal. By this time, the fetus is often dead, and signs of infection in the fetal membranes or fetus may be evident.
Prognosis
The prognosis is good in most cases that are diagnosed early.
Clinical Signs
- Preparations for birth begin but do not continue into second-stage labor.
- The fetus is normally in the correct presentation, position, and posture.
- The cervix is dilated or easily dilatable with manual pressure but there is no evidence of uterine contractions.
- The fetal membranes, especially the amnion, are often still intact.
- In cases of hypocalcemia the patient will be dull, reluctant or unable to rise, and have a low temperature, dilated pupils, and reduced rumenal activity. The is turned back to the flank and, if untreated, the cow may become comatose with death ensuing.
- In cases of hydrops uteri there will probably have been a history during pregnancy of increasing abdominal size and debility.
- If accessible the uterine wall is found to lack muscle tone when palpated.
Treatment
If hypocalcemia is suspected, intravenous treatment with 450 ml of either 20% or 40% calcium borogluconate solution should be administered. An additional 400 ml of the same solution can be given subcutaneously.
If there is a history of concurrent magnesium deficiency on the farm, a 400 ml injection of a calcium-magnesium-phosphorus-dextrose solution should be given intravenously. In many cases, parturition will resume, but delivery should be assisted with moderate traction, as is recommended in cases of uterine inertia from other causes. Failure to deliver the calf promptly may result in its death due to placental separation.
After the fetus is removed, 20 IU of oxytocin should be administered intramuscularly to promote uterine involution and expulsion of the placenta.
Secondary Uterine Inertia
Secondary uterine inertia is characterized by exhaustion of the uterine muscles, which results from or follows dystocia. It is observed across all species.
In multiparous animals, it may occur even after dystocia involving just one fetus; the remaining fetuses may not be expelled once the fetus causing the dystocia has been removed.
Certain “sensitive” dams may refrain from vigorous labor due to pain, leading to secondary inertia.
In other multiparous animals that lack adequate body condition or strength, several young may be delivered initially, after which both the dam and the myometrium appear exhausted.
Secondary inertia is frequently followed by uterine infections, septic metritis, retained placenta, and a failure of normal uterine involution.
In cases of prolonged dystocia in uniparous and possibly multiparous animals, the uterine muscle may become fatigued, leading to the formation of contraction or retraction rings, also known as Bandl’s rings. These rings may contract tightly around the fetus or caudal to it, complicating the relief of dystocia. If unrecognized, this may result in uterine rupture during forced extraction of the fetus.
In certain dog breeds, such as the Scotch Terrier or Dachshund, secondary uterine inertia may occur spontaneously early in the second stage of parturition. Typically, one or two fetuses are expelled normally, after which labor ceases despite the presence of additional fetuses in the uterus.
Prognosis
Prognosis in secondary uterine inertia is more guarded than in primary uterine inertia because the fetuses may be weak, dead, or emphysematous, and rupture of the uterus is more common. Retained placenta and metritis are usual sequelae.
Treatment
The primary cause of dystocia should be addressed first, followed by delivery of the fetus. Uterine involution is encouraged post-delivery with an injection of oxytocin, as in cases of primary uterine inertia.
When managing this type of dystocia in large animals, the condition causing the obstruction should be corrected—if possible—through mutation, and the fetus should then be removed using moderate, careful traction.
Lubrication of both the fetus and the birth canal is usually necessary.
Excessive traction must be avoided, especially in the presence of strong contraction or retraction rings, as they can significantly hinder fetal removal and may result in transverse uterine rupture.
If the contraction rings are not too tight, slow, cautious mutation and traction may successfully relieve the dystocia. However, in severe cases where the rings greatly reduce the uterine lumen or diameter, fetotomy or caesarean section may be required to resolve the condition.
Since uterine infection is commonly present in these cases, a ventral abdominal approach is recommended for performing the caesarean operation.
Uterine inertia is a significant cause of dystocia in animals and requires early diagnosis and timely intervention. Understanding its types, causes, and treatments is crucial for improving maternal and fetal outcomes in veterinary practice.
FAQs
Uterine inertia is the failure of the uterus to contract properly during or after parturition, leading to delayed or failed delivery.
The two types are primary uterine inertia (failure to initiate contractions) and secondary uterine inertia (exhaustion of uterine muscles after prolonged labor).
Treatment includes correcting calcium or magnesium deficiencies, administering oxytocin, and assisting delivery with traction or cesarean if necessary.