TABLE OF CONTENTS
Upward Fixation of the Patella in Horses
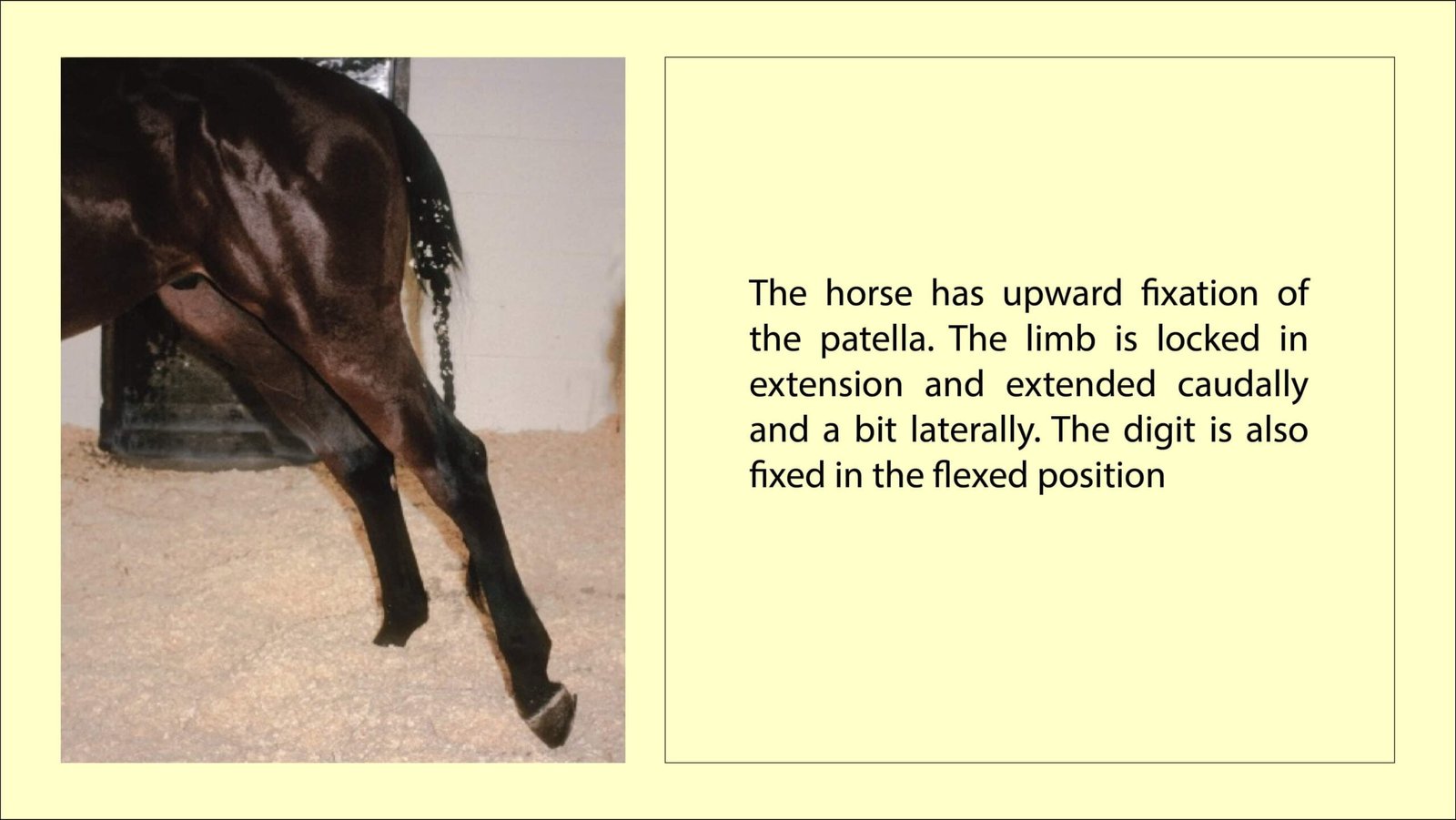
Upward Fixation of the Patella (UFP) in Horses occurs when the medial patellar ligament (MPL) becomes caught over the medial trochlear ridge. If it becomes fixed in that position, the hindlimb cannot be flexed and the horse assumes a posture with the affected limb extended in a caudally abducted position with the fetlock flexed due to the reciprocal apparatus.
The horse has upward fixation of the patella. The limb is locked in extension and extended caudally and a bit laterally. The digit is also fixed in the flexed position
Etiology
Upward fixation of the patella generally has been considered to occur in horses that have exceptionally straight hindlimbs.
Body type is strongly inherited, thus it is likely that the tendency for UFP could be congenital. Shetland ponies are particularly affected, and UFP predisposes them to coxofemoral luxation.
The condition also appears when the medial patellar ligament becomes long enough to reach over the medial trochlear ridge in spite of normal conformation. Examples of this include loss of quadriceps muscle tone and traumatic hyperextension of the hindlimb. The ligaments may become stretched once upward fixation occurs, so recurrence is common.
The MPL is weaker than the other 2 patellar ligaments. Furthermore, younger horses, when they begin training, often lack the muscle tone they will acquire as they work. Upward fixation also has been observed in horses abruptly taken out of training and confined to a stall.
Clinical signs and Diagnosis
In acute upward fixation of the patella, the hindlimb is locked in extension, as described above. The condition may relieve itself, or it may remain locked for several hours or even days.
In other cases, there is only a “catching” of the patella as the horse walks.
Hyperextending the stifle by walking down an incline may cause a jerking gait from intermittent catching of the MPL, and the horse may assume a crouched position, presumably to prevent stifle extension.
Backing or moving in a tight circle also exacerbates the signs.
When the MPL releases, the hindlimb usually jerks up quickly, mimicking stringhalt. UFP must be differentiated from stringhalt.
Both hindlimbs usually are predisposed to the condition; however, truly unilateral cases often have a history of an inciting cause in the affected limb.
Palpation when the limb is locked in extension reveals tense patellar ligaments and that the patella is locked above the medial trochlear ridge of the femur.
The horse drags the front of the hoof on the ground when it is forced to move forward with the limb locked.
When the limb is in a normal position, the predisposition can be evaluated by forcing the patella upward and outward with the hand. If the limb can be manually locked in extension for 1 or more steps, it is predisposed to UFP; manual induction of UFP should not be possible in a normal horse. The examiner should take care not to be in the path of the limb when it releases.
Lameness usually is not severe or constant, but femoropatellar synovitis and distention may occur with repeated episodes.
Coxofemoral strain may be associated with persistent UFP, as well.
Radiographs of the stifle should be taken to eliminate conditions that predispose to UFP. Although uncommon, hypoplasia of the medial trochlear ridge, such as occurs with OCD, facilitates the displacement. Most affected horses do not have radiographic changes from intermittent UFP.
Treatment of Upward Fixation of the Patella in Horses
For a persistently fixed patella, a sideline may be applied to the affected limb so that as the limb is drawn forward, the patella is pushed medially to unhook the MPL, and downward, which often disengages the fixed patella.
Backing the horse may also dislodge the patellar ligament. Personnel should take care to be out of the range of the “jerk” when the MPL releases.
Many horses respond to controlled conditioning to increase quadriceps strength and tone, which tightens the MPL. However, if the horse’s fitness level drops below optimal, the UFP recurs. Obviously, rest or confinement is contraindicated.
Conditioning, including going up hills without coming back down the incline, which exacerbates the hyperextension of the stifle, strengthens and tones the quadriceps.
If conditioning and/or shoeing fails to halt the incidence of upward fixation of the patella, the MPL can be tightened with scar tissue by creating a series of longitudinal incisions in the MPL. This substantially thickens the MPL and presumably causes a functional shortening and tightening of the MPL. The advantage of this procedure compared to MPD is that the patella remains stable.
A much older treatment that has been commonly used for horses with intermittent upward fixation and no palpable swelling of the femoropatellar joint capsule is the injection of counterirritants into the middle and medial patellar ligaments. The injections are usually performed on the standing horse using mild sedation and nose twitch. Commonly used irritants contain 2% iodine; 1 to 2 ml is injected in 6 equally distributed sites along the medial patellar ligament. Most horses exhibit a slight stiffness and swelling for a few days after the injections. Daily mild exercise is recommended so there is minimal loss of muscle tone. While most horses respond well to this treatment, a few require re-treatment.
When nothing else helps or the UFP cannot be reduced, an MPD is performed using local anesthesia in the standing horse.
To perform the procedure in the standing horse, a 1-cm incision should be made along the medial limit of the middle patellar ligament near its tibial attachment. A curved mosquito hemostat is inserted and dissected axial to the medial patellar ligament. A Udall’s teat bistoury, or other suitable blunt bistoury, is inserted along the path created with the blade directed distally. The tip of the bistoury is palpated subcutaneously in the same position caudal to the medial patellar ligament as the hemostat was just palpated. Once the medial patellar ligament has been transected, determination of remaining MPL vs. gracilis/ sartorius aponeuroses can be difficult, although transection of some of those fibers may not be a problem (see below). The horse should be kept in the stall, with hand walking gradually increasing over a period of 90 days. From that point a conservative conditioning program for regular work can begin.
An alternative procedure performed with the horse under general anesthesia in dorsal recumbency has been described. It is similar to the above procedure except the incision is continued into the aponeuroses of the gracilis and sartorius muscles until the limb can be fully extended and flexed without resistance or catching.
Prognosis
The prognosis is good for horses that respond to a conditioning program and maintain that fitness level. After conditioning and ensuring correct shoeing, the logical progression is counterirritant injection, medial patellar ligament splitting, and then medial patellar ligament desmotomy. The diagnosis should be confirmed before surgery is performed because more complications have appeared when MPD is performed on unaffected horses.