TABLE OF CONTENTS
Retained Fetal Membranes (RFM) in Mares
Retained fetal membranes (RFM) in mares is potentially more serious affection than the same in cattle.In horses, RFM should be treated as an emergency.
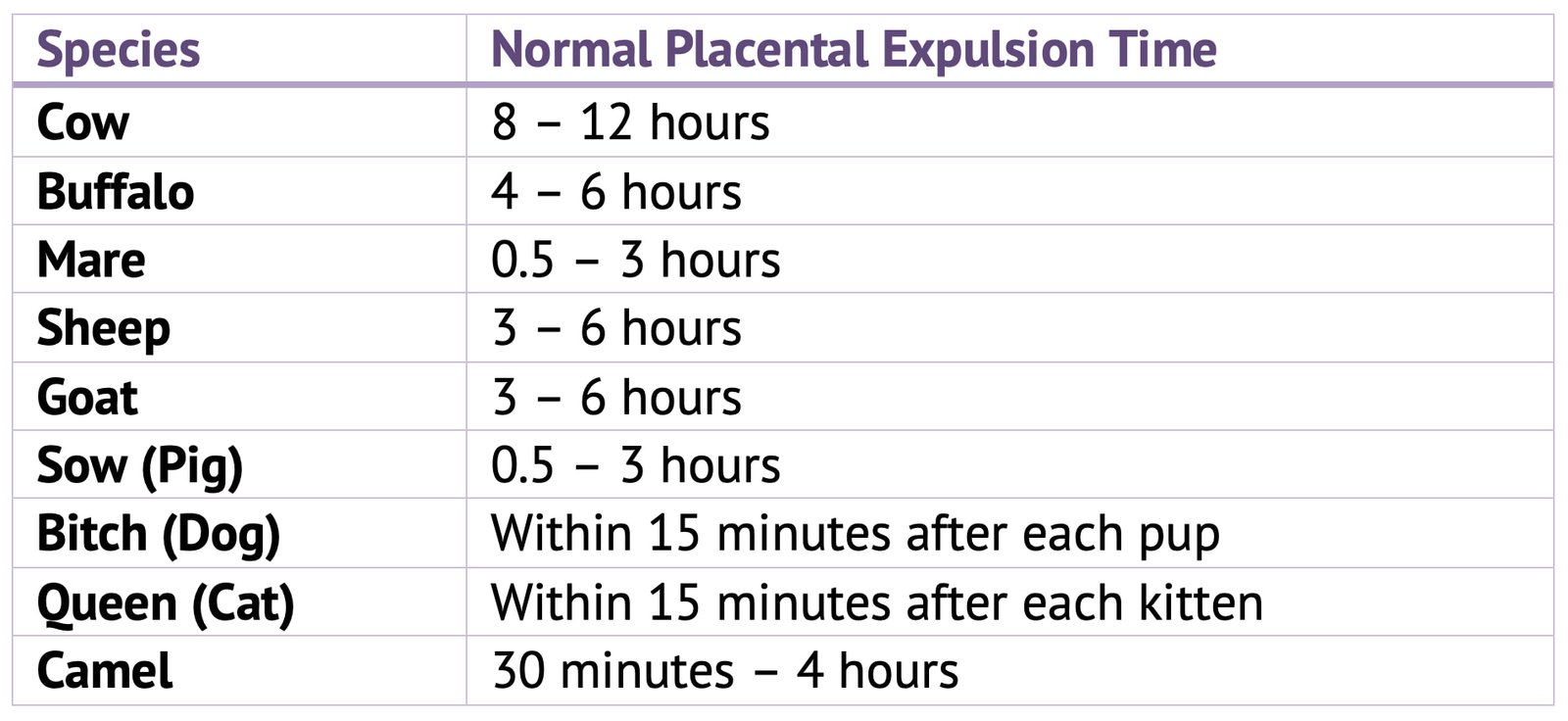
The average time taken for the fetal membranes to be expelled is about 1 hour, and should not exceed 2 hour, although there is debate amongst equine clinicians about the latter.
Clinical Signs
- Most obvious sign is presence of a variable portion of tissue protruding from the vulva; less commonly nothing is visible.
- Either this means that no parts of the fetal membranes have been expelled or, more likely, portions remain attached.
Complications
- Complications include acute metritis, septicaemia, laminitis and even death.
- With prompt and effective treatment these sequelae can be avoided.
- In many cases, uterine involution is delayed even if these more serious complications do not develop.
Treatment
- Initially, the protruding membranes should be tied in a knot to prevent them touching the hocks.
- As uterine contractility plays an important role in the dehiscence of the fetal membranes, administration of oxytocin is recommended as a first and most successful method of treatment in up to 90% of cases.
- It is a good rule not to wait longer than 6 hours after delivery of the foal; the time interval should be shorter in heavy breeds. This method of treatment avoids manipulation within the uterus, with the risk of introducing microorganisms.
- Oxytocin can be given via the intramuscular route (20-40 IU), which can be repeated after 1 hour if the membranes have not been expelled. Alternatively, use slow intravenous infusion of 50 IU oxytocin in 1 litre of physiologic saline over 1 hour. Symptoms of colic often follow injections of oxytocin and commonly precede natural expulsion so that pain relieving drugs and sedation may be required.
- Attempt gentle removal only in cases where treatment is unsuccessful and the membranes are almost detached but retained within the uterus. Removal of placenta should be carried out with scrupulous regard to asepsis, and no undue force should be applied, for even moderate traction on the afterbirth may cause the uterus to become inverted and prolapsed.
- In most cases of retention, some separation of the allan to chorion has occurred and consequently a variable amount of the afterbirth hangs down from the vulva.
Manual Removal of Retained Fetal Membranes
- The mare is effectively restrained and measures should be taken to protect the operator from being kicked.
- The tail is bandaged and held to one side by the attendant while the obstetrician thoroughly washes the perineum and rear of the mare.
- With the hand and arm protected by a clean plastic sleeve, the extruded mass, or failing that the freed part lying within the vagina, is grasped and twisted into a rope
- The gloved hand anointed with lubricant is gently introduced along the ‘rope’ to the area of circumferential attachment in the uterus.
- As the ‘rope’ is gently pulled and twisted, the tips of the fingers are pressed between the endometrium and the chorion.
- The villi are easily detached, and as the allantochorion is gradually freed it is taken up by further twisting of the detached mass.
- The allantochorionic membrane is gently separated from the endometrium by moving one of the hands between them.
- The tightest attachment is usually at the tip of the horn.
- The process of separation usually goes quite smoothly, and the complete sac of allantochorion can be gradually detached from the pregnant horn.
- There is a tendency for attachment to be firmer in the non-pregnant horn, and occasionally retention is confined to this horn.
- If it is found impossible to detach the apical portions of the allantochorionic sac without tearing the membranes it is better to desist and to try again in 4-6 hours, by which time a successful outcome will be likely.
- Unwanted side-effects of this manual removal may be serious haemorrhage, invagination of one of the horns and a higher chance of retention of microvilli in the endometrium.
- Vandeplassche and his colleagues (1971 and 1972) refer particularly to the residue of microvilli that is present in the endometrium even after a normal expulsion of the after birth and is vastly increased when manual removal is effected in a case of retention.
- During a difficult manual removal only the central branches of the chorionic villi are removed while practically all the microvilli are broken off and retained; rupture of endometrial and subendometrial capillaries may also occur.
- The consequences of the difficult removal such as increased puerperal exudate, containing much tissue debris; endometritis and laminitis; uterine spasm and delayed involution of the uterus. It is for these reasons they prefer to treat severe equine retention by means of intravenous drip administration of oxytocin rather than by persistence with manual removal.