TABLE OF CONTENTS
Quittor in Horses
Quittor in Horses is the term used to describe chronic purulent inflammation of a collateral cartilage (ungual) of the distal phalanx characterized by cartilage necrosis and multiple fistulous draining tracts proximal to the coronary band. The lateral cartilages of the forelimb are most commonly affected.

Etiology
Infection and subsequent necrosis of the collateral cartilage is usually caused by a direct injury to the cartilage or to the soft tissues overlying the cartilage.
Injuries to the collateral cartilage that predispose to quittor include penetrating wounds and lacerations, external blows that bruise and damage its blood supply (e.g., interference), foot abscesses, chronic ascending infections of the white line in the quarters, and deep hoof cracks that result in localized infection in the collateral cartilage.
Clinical Signs
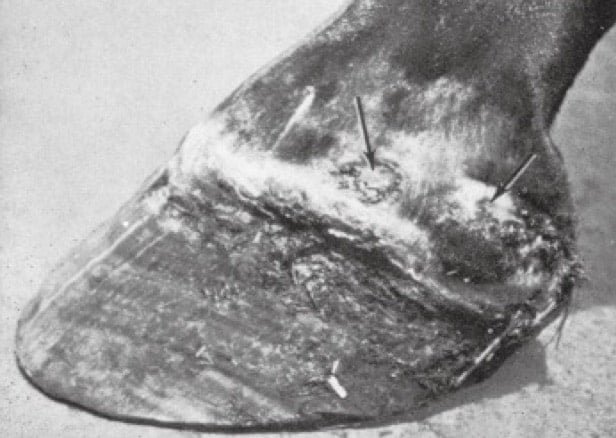
- Quittor in Horses is characterized by the formation of abscesses within the collateral cartilage which break open and drain just proximal to the coronary band.
- A history of recurrent drainage from fistulous tracts overlying the affected cartilage and intermittent severe lameness is common.
- Swelling, heat, and pain with pressure over the affected cartilage are often present.
- Pain is usually elicited with hoof testers over the affected quarter. The degree of lameness is usually affected by the patency of the fistulous tract draining the abscesses.
- Lack of drainage increases pressure within the abscess, often resulting in severe lameness.
- Once the abscess breaks open and drains, the lameness usually subsides.
- Chronic inflammation of the involved cartilage may cause permanent hoof damage resulting in deformity of the foot and persistent lameness.
Diagnosis
- The diagnosis is usually based on a history of recurrent swelling of the affected collateral cartilage, the presence of 1 or more fistulous tracts proximal to the coronary band, and intermittent lameness.
- Swelling and pain over the affected cartilage supports the diagnosis.
- Quittor should be differentiated from shallow abscesses and ascending infection of the white line (gravel). The drainage tract associated with gravel is usually located at or just proximal to the coronary band, and the inflammatory process is often localized.
- With quittor there may be multiple fistulous tracts, and the swelling is usually more diffuse and located more proximally over the collateral cartilages.
- Radiographs can be used to rule out bone involvement but lysis of the collateral cartilage associated with infection cannot be seen on radiographs.
- However, osteomyelitis of an ossified collateral cartilage can occur.
- The depth and dimension of the draining tract(s) can also be determined with fistulography or by placing a sterile flexible metal probe within the tract.
Treatment
- The treatment of choice is surgical excision of the fistulous tract(s) and necrotic cartilage.
- Medical management with systemic antibiotics, foot soaks, and injection of the fistulous tracts with antiseptics is usually not effective because of the limited blood supply to the cartilage.
- Medical treatment may temporarily suppress the infection but often just delays the eventual need for surgery.
- However, improved medical treatment of these infections may be obtained with IV regional perfusion of antimicrobials.
- At surgery the foot should be held in rigid extension by placing traction with wires placed through holes drilled in the hoof wall.
Prognosis
The prognosis for most cases of quittor following complete excision of the necrotic cartilage is good unless the infection is very chronic.
Secondary complications such as osteomyelitis of the distal phalanx, septic arthritis of the DIP joint, or infection of the digital cushion or other soft tissues in the foot reduce the prognosis appropriately.