TABLE OF CONTENTS
Pedal Osteitis
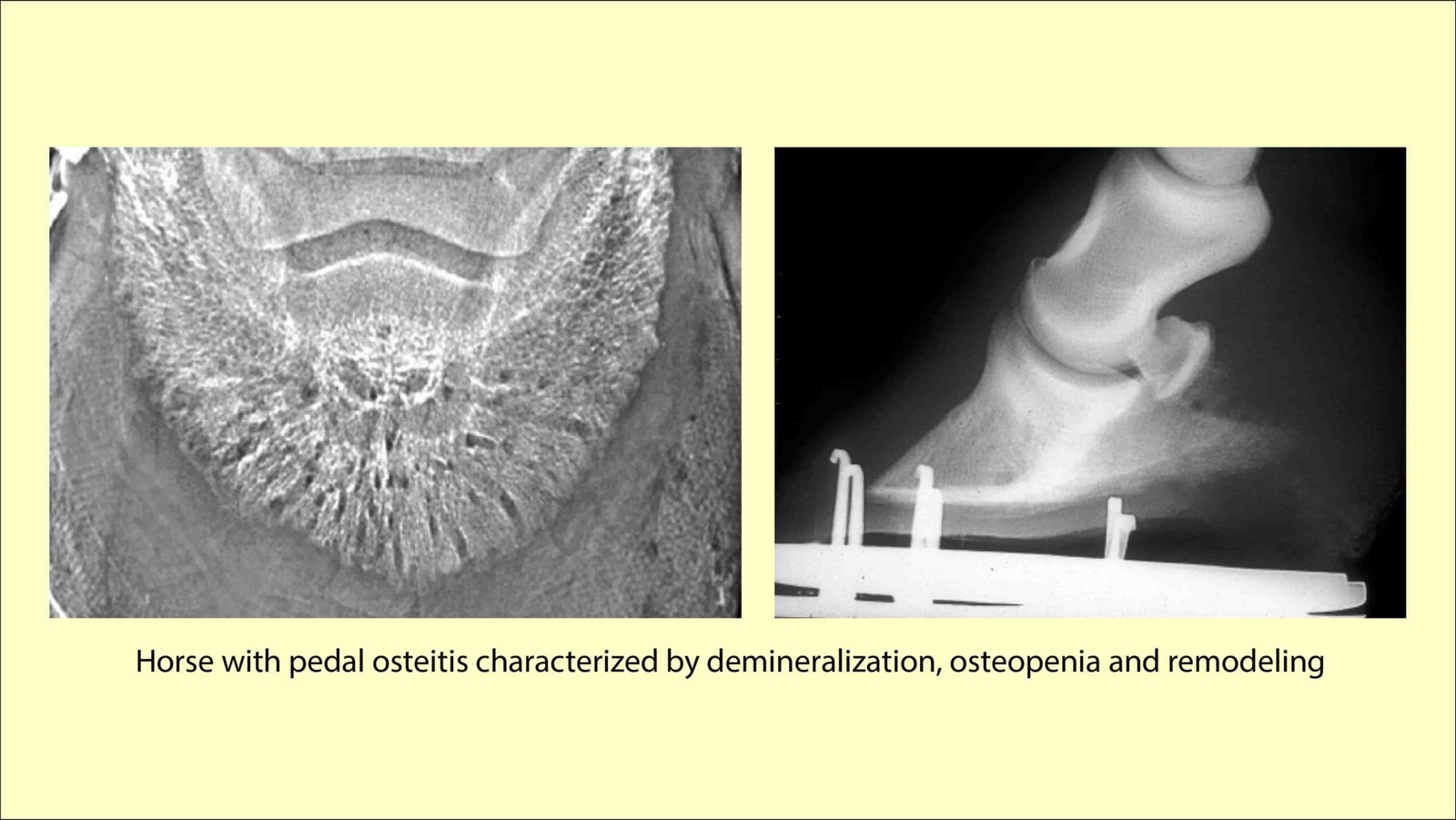
Pedal osteitis (PO) is defined as an inflammatory condition of the foot that results in demineralisation of the distal phalanx. Radiographically the condition appears as a focal or diffuse radiolucency of the bone or as new bone formation.
The two recognized classifications of pedal osteitis are non-septic and septic. The distal phalanx does not have a medullary cavity so inflammation of this bone is referred to as osteitis rather than osteomyelitis.
Etiology
Non-septic Pedal Osteitis is a poorly defined disorder of the distal phalanx that may occur as a primary condition or develop from a secondary cause.
Primary PO is usually associated with severe or chronic sole bruising resulting from repeated concussion during exercise on hard surfaces.
Secondary causes of nonseptic PO include persistent corns, laminitis, penetrating wounds, bruised soles, and conformational faults.
Septic PO refers to bacterial infection within the distal phalanx. Environmental microbes gain access either by direct introduction of the microbes into the distal phalanx (e.g., deep penetrating wound), extension of infection from the soft tissues of the foot into the distal phalanx, or from hematogenous sources in foals.
Clinical Signs
Non-septic PO most commonly affects the forelimbs, and the condition may be unilateral or bilateral. The severity of the lameness is variable and depends on the cause and degree of injury.
The lameness may be accentuated after exercise, work on hard surfaces, or directly after trimming and shoeing.
Hoof tester examination often reveals focal or diffuse sensitivity of the sole at the toe region. However, the entire sole may be painful.
Perineural anaesthesia of the PD nerves usually eliminates the lameness. Septic PO occurs most commonly in the forelimbs in adult horses and in the hind limbs in foals.
The severity of lameness in horses with septic PO is usually greater than that seen with nonseptic PO.
Diagnosis
- Radiographic assessment of the distal phalanx for the presence of non-septic PO should include at least three views–
- 60° dorso palmar and the medial and lateral oblique projections.
- The radiographic signs associated with non-septic PO include-
- Demineralization,Widening of the nutrient foramina at the solar margin, and
- Irregular bone formation along the solar margins of the distal phalanx.
Treatment
Treatment of non-septic PO often depends upon the inciting cause, use of the horse, and environmental factors.
- In general, treatment is aimed at reducing the inflammation within the distal phalanx, minimizing concussion to the foot, and eliminating the inciting cause-
- Corrective shoeing
- Oral NSAIDs and Rest
A wide web egg-bar shoe whose solar surface is deeply concaved has been recommended to prevent the injured sole from contacting the ground.
Alternatively, shoes with rim pads can be applied to reduce concussion and protect the injured sole.
The toe of the shoe can be squared or rolled to enhance break-over
Thin and soft soles can be medicated topically with equal parts of phenol, formalin, and iodine to “toughen” them.
A prolonged rest period is usually only necessary if a solar margin fracture is present or if the lameness is severe. Rest and avoiding exercise on hard surfaces are usually indicated until the lameness subsides.
Exercising on softer track surfaces, such as wood chips, or swimming the horse to maintain fitness may allow the horse to continue training until the lameness resolves.
Treatment of septic PO usually involves systemic and local antimicrobials (regional limb perfusion) and surgical debridement of the infected bone.
Regional IV limb perfusions can be repeated after surgery to help treat the infection
Prognosis
The prognosis for non-septic Pedal Osteitis is often very good if the condition is of a relatively short duration and the exercise environment can be controlled.
It is less favorable if the disease is chronic and the horse must continue to compete on hard surfaces, or if the condition is secondary to chronic laminitis.
The prognosis for horses with septic PO appears very good to excellent if the infection can be controlled.