TABLE OF CONTENTS
Opioids drugs in animals
Opioids drugs in animals are commonly used as narcotic analgesics. Narcotic is a Greek word used for stupor and this word narcotic is most appropriately used for any drug that induces sleep.
Opium has been used in medicine since the dawn of history. Opium is the air-dried milky exudates obtained from the incised unripe seed capsules of the poppy plant Papaver somniferum.
Opium contains about 24 alkaloids but only a few like morphine and codeine are of importance. The alkaloids may be phenantherenes like morphine, codeine and thebaine or benzylisoquinolines like papaverine and noscapine. The term opioid is applied to any substance, whether endogenous or synthetic, that produces morphine-like effects that are blocked by antagonists such as naloxone.
The older term, opiate, is restricted to synthetic morphine-like drugs with non-peptidic structures. Tincture of opium is known as laudanum and camphorated tincture of opium is known as paregoric. Paregoric is used in the treatment of diarrhoea.
Chemistry of Opioids drugs
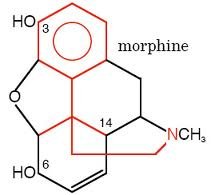
Morphine was the first plant alkaloids that was isolated. Morphine molecule consists of a partially hydrogenated phenantherene nucleus. In addition two hydroxy groups (alcoholic and phenolic) are important in maintaining the pharmacological integrity of the morphine molecule.
Alteration in the phenolic hydroxy group reduces analgesic potency, respiratory depression and likelihood of constipation. A stimulant activity upon the CNS is noted when substitution is made in this position.
If substitution is made in the alcoholic hydroxy position, narcotic and respiratory depressions are enhanced. Eg: Hydromorphone. Substitution in either of the hydroxy positions lessens the emetic activity of the parent molecule. Codeine and hydromorphone are less potent than morphine in producing emesis.
Semisynthetic derivatives of morphine are apomorphine hydrochloride, a potent emetic agent and naloxone hydrochloride, an antagonist of opiate drugs that have important clinical applications.
Mechanism of action of opioids
Opioids act centrally to elevate the pain threshold and to alter the psychological response to pain. They also act peripherally. The pharmacological effects result from interactions with one or more of the four opioid receptors (mu, sigma, kappa and delta).
The pharmacological effects vary among the opioid derivatives, depending upon the physiological effects associated with each receptor, its location in the body and the type of interaction between the opioid and the receptor.
- Opiate receptors occur in high density in the dorsal horn of the spinal cord, where they are responsible for modulating pain-
- μ (Mu) receptors give rise to analgesia and sedation above the spinal cord or in the spinal cord. Interactions with μ receptors also cause euphoria, respiratory depression and physical dependence.
- κ (Kappa) receptors are responsible for analgesia that is spinal in origin and for miosis and sedation.
- σ (Sigma) receptors are no longer recognized as a separate class of receptors. Positive interactions between drugs and these receptors provide no analgesia. Rather, many of the adverse effects of the opioids are mediated at these receptors, including dysphoria, hallucinations, respiratory stimulation and some of the vasomotor responses to opioids.
- δ (Delta) receptors appear to modulate, among other effects, emotional behaviour and immunomodulation. These receptors may also contribute to analgesia.
All opioid receptors are linked through G-protein to inhibition of adenylate cyclase. They also facilitate opening of potassium channels causing hyperpolarization and inhibit opening of calcium channels. These membrane effects are not linked to decreased cAMP formation.
Species differences in number of receptors, their location and specificity and selectivity to the various drugs are important to differences in response to the opiates.
Opioids can interact with these receptors as agonists or antagonists. Pure agonists have high affinity for delta and kappa sites. Some drugs like codeine, methadone and dextropropoxyphene are referred to as weak agonists, since, their maximal effects, both analgesic and unwanted side effects are lower than those of morphine and they do not cause dependence.
Mixed agonists exhibit variable binding specificities at each receptor sub type, with some sites being agonistic and other sites antagonistic. Partial agonists do the same as mixed agonists, but their positive interaction with the receptors occurs with less than full activity at some of the receptors. Thus many of the varied effects of these drugs result from the agonistic actions at one receptor and antagonistic activity at another.
Endogenous opioids
Three families of endogenous opioids have been described. They are β endorphins, enkephalins and dynorphin. β endorphins are present in the pituitary gland, hypothalamus, small intestine, placenta and plasma. Enkephalins are widely distributed in areas of the CNS that receive afferent nociceptive information. They also exist in the peripheral nervous system, gastrointestinal tract and plasma. Dynorphins are believed to function primarily as neuromodulators in the CNS through interaction with the mu, kappa and delta opioid receptors.
The greatest role of β endorphins is probably modulation of nociception during stress and acupuncture.
Enkephalins act as inhibitory neurotransmitters and may elicit analgesia through the modulation of substance P release. Enkephalins play a role in acupuncture mediated, analgesia.
Dynorphins may be most important in nociception at the spinal cord level through activation of kappa receptors.
Pharmacokinetics of opioids
- Readily absorbed from GI tract, nasal mucosa, lung, subcutaneous, intramuscular and intravenous route
- Wide distribution
- Has wide volume of distribution
- Free morphine accumulates in kidney, lung, liver, and spleen
- CNS is primary site of action (analgesia/sedation) – Biotransformation in liver – Conjugates with glucuronic acid
- Excreted by kidney
- Half life is 2.5 to 3 hours (does not persist in body tissue)
Pharmacological effects of morphine
Antinociception by morphine
Severe cancer pain is tolerated more when morphine is given; relieves all types of pain, but most effective against continuous dull aching pain- sharp, stabbing, shooting pain also relieved by morphine.
- When morphine is given to a pain free individual-
- Morphine causes miosis (pinpoint pupils) due to kappa receptor effect
- Pinpoint pupils show still responsive to bright light
- Oculomotor nerve (Cranial Nerve 3) is stimulated by kappa receptor site
- If kappa receptor is blocked, mydriasis from sigma effect will result
- Atropine partially blocks effect indicating parasympathetic system involved
- High doses (overdose situation) of morphine cause excitatory and spinal reflexes
- High doses of many OPIOID agents cause convulsions due to stimulation at sigma receptor
CNS effect by morphine
Central nervous system is the primary site of action of morphine. Morphine causes sedation effect, with no loss of consciousness, analgesia, euphoria, mood change mental cloudiness. depending on the dose and its primary and continuous depression of respiration leads to : decrease rate, decrease volume and decrease tidal exchange.
CVS effect by morphine
- Morphine produces vasodilatation
- Morphine causes the release of histamine and
- Suppression of central adrenergic tone and
- Suppression of reflex vasoconstriction
GI tract effect by morphine
- Increase in tone and decrease in mobility leads to constipation
- Decreased concentration of HCl secretion
- Increased tone in stomach, small intestine, and large intestine delay of passage of food (gastric contents) so more reabsorption of water leading to constipation effect.
On smooth muscles
- Biliary tract – marked increase in the pressure in the biliary tract
- Increase due to contraction of Sphincter of Oddi urinary bladder
- Tone of detrusor muscle increased, feel urinary urgency
- Have urinary retention due to increased muscle tone where sphincter closed off
Bronchial muscles
Bronchoconstriction can result, Contraindicated in asthmatics, particularly before surgery.
Uterus
Contraction of uterus can prolong labor by using of morphine drug.
Neuroendocrine effect of morphine
Inhibit the release of gonadotropin-releasing hormone (GnRH) and corticotropin-releasing factor (CRF) and Decreasing circulating concentrations of luteinizing hormone (LH), follicle-stimulating hormone (FSH), ACTH, and beta endorphin. TSH unaffected.
Synthetic opioids
Codeine
- Substitution of hydroxyl moiety with methyl group on 3 position
- Analgesic potency is one tenth the potency of morphine
- Absorbed readily from GI tract,the absorption is more regular and predictable than morphine
- Metabolized like morphine through glucuronic acid
- Physical dependence is necessity of drug so you don’t go through withdrawal
- Tolerance and physical dependence is protracted from morphine since potency of codeine is low
- Withdrawal from codeine is mild in relation to morphine
- Antitussive
Heroin (diacetylmorphine)
- Substitution with acetyl groups at 3 and 6 hydroxy positions
- Analgesic potency is 3 to 4 times more of morphine
- Most lipophilic of all the OPIOIDs
- Morphine is the least lipophilic of all the OPIOID
- Crosses the blood brain barrier rapidly (morphine crosses slowly)
- Hydrolyzed to mono acetyl morphine, then to morphine making more of the drug in the brain making it 3 to 4 times more potent withdrawal symptoms of heroin similar to morphine, but more intense (rebound effect, mydriasis, diarrhea, vasoconstriction, dysphoria etc.)
Hydromorphone
- Substituted with ketone at 6 hydroxyl position of morphine
- Strong agonist
- Highly potent
- More sedative than morphine so less euphoric
- Less constipation
- Does not produce miosis
- Tolerance and physical dependence is more intense than morphine because of its high potency
- Respiratory depression
Fentanyl
- Synthetic drug
- More potent than morphine
- Rapidly acting
- Used as preanaesthetic medication
- Short acting (30-45 min)
- Onset of action is 5 minutes
- Very highly potent
- Highly abused – known as china white as street name
Meperidine
- Addictive liability as morphine
- CNS effective actions as morphine
- Sedation, analgesia, respiratory depression
- Highly potent as morphine
Uses of opioids
- Morphine is the prototype drug – Morphine from opium – dried latex from the unripe capsule of Papaver somniferum- The ‘gold standard’ for assessing analgesics
- Analgesia – euphoria – respiratory depression – vomition – constipation by increasing the tone of the gut ( closure of lumen and also the sphincters)
- Man, dog and rabbits – depression
- Cats and horses – stimulation
- Miosis in dogs and mydriasis in cats
- Little effect on CVS – higher doses may cause bradycardia
- Use – analgesia before, during and after surgery- eg., Codeine, Diacetylmorphine (Heroin) – acts as agonist: Nalorphine, lavallorphan acts as partial agonist and Naloxone as pure antagonist.
- Pethidine – 1/10th as potent – spasmolytic, analgesic, sedative
- Methadone – synthetic agonist – equipotent – used in horses and dogs
- Fentanyl – 50 times as potent -Part of neuroleptanalgesia, balanced anaesthesia and for postoperative analgesia (transdermal patches – for prolonged pain relief)
- Pentazocine – analgesic- prescription drug
- Buprenorphine – partial agonist – slower onset and long duration of action (bell shaped curve for analgesia) higher doses poor analgesia
- Etorphine– very potent – needs a very small dose – (0.5 mg / 500 kg)
- Small volume enough to sedate and anaesthetize large animals using dart guns – very long acting
- Immobilon for neuroleptanalgesia ( + acepromazine or methotripromazine)
- Diphenoxylate – antidiarrhoeal
- Codeine – cough suppressant
- Naloxone – antagonist – used to reverse toxicity or delayed sedation.
Opioid drug interactions
- Opioids and phenothiazines
- produces an additive CNS depression as well as enhancement of the actions of OPIOID (respiratory depression)
- Produce a greater incidence of orthostatic hypotension
- Opioids and tricyclics antidepressants -Produce increased hypotension
- Meperidine and MOA inhibitors – results in severe and immediate reactions that include excitation, rigidity, hypertension, and severe respiratory depression
- Opioids and barbiturates – increased clearance of opioids
- Opioids and amphetamine – enhanced analgesic effect
Species differences and toxicity of opioids
Equine, Bovine, Caprine, Ovine, Porcine, and Feline patients may show CNS stimulation rather than CNS depression. Canine patients may initially defecate with the opioids. This is frequently followed by decreased GI motility, leading to constipation that is more commonly associated with this class of drugs.
Dogs may also respond to opiates with initial respiratory stimulation, which is then followed by typical respiratory depression. The opiates are cough suppressants in dogs. Additionally, dogs will exhibit coronary vasoconstriction, the opposite effect of that observed in humans.
Rabbits, Canines (and primates) exhibit miosis (pupillary constriction) while feline and other species exhibit mydriasis (pupillary dilatation). Canine and feline patients will exhibit emesis at very high doses, while other species (especially ruminants and swine) do not exhibit emesis.
Dogs and rabbits will typically exhibit hypothermia in response to the opiates while cattle, goats, horses, and cats typically exhibit hyperthermia.
The opiates are used primarily as analgesics in veterinary practice, often administered with an ataractic (such as acepromazine), especially in excitable species.
Absorption, fate and excretion
Opioids are readily absorbed from the small intestine and some from the stomach. Absorbed well after subcutaneous administration. Not absorbed through intact skin. Glucuronide conjugation is the primary metabolic pathway.
Toxicity
Toxicity decreases with maturity of the animal. In dogs convulsions similar to strychnine are noticed. In cattle CNS stimulation and gastrointestinal disturbances without fatality. Addiction is rarely encountered in animals.
Precautions and contraindications
Tolerance develops to morphine usage. High degree of tolerance is exhibited in analgesia, euphoria, sedation, respiratory depression, antidiuresis, emesis and anti tussive, moderate tolerance is exhibited in bradycardia and no tolerance is exhibited in miosis and constipation.
Used with caution in uremic and toxemic dogs. Should not be used to control strychnine poisoning, tetanus and epilepsy. Should not be administered in shock and in animals with head injury.
Opioid antagonists
Naloxone
- No analgesic activity at all
- Competitive antagonist at mu, kappa, and sigma receptor
- Displaces morphine and other OPIOID from receptor site
- Reverses all actions of the OPIOID and does it rather quickly
- Precipitate withdrawal person on heroin
- Naloxone effects are seen in the first five minutes and it only lasts for 30 minutes:
- Increase blood pressure
- Metabolized same as morphine through glucuronic acid and excreted through kidney
Naltrexone
- Almost similar to naloxone except it is used orally
- Long duration of activity
- Single dose block action of heroin effects for 24 hours
- Used for emergency treatment
- Once stabilized, give patient naltrexone
- Patient get no euphoric effect from heroin so person gets off heroin (negative reinforcement)
- Approved for use by the FDA
- Also used for treatment of alcohol rehabilitation