TABLE OF CONTENTS
Malignant Catarrhal Fever (MCF)
Malignant Catarrhal Fever (MCF) also known as Malignant head catarrh, Snotsiekte, Catarrhal fever, Gangrenous coryza.
Malignant catarrhal fever (MCF) is an acute, generalized and usually fatal disease affecting many species of Artiodactyla.
Malignant Catarrhal Fever (MCF) is characterized by lymphoid cell accumulations in non lymphoid organs, vasculitis and hyperplasia of T lymphocyte in lymphoid organs. MCF usually appears sporadically and affects few animals in the population.
Etiology
- Alcelaphine herpes virus-1 (AlHV-1)- Wildebeest associated malignant catarrhal fever virus of the genus Maca virus.
- Ovine herpes virus-2 (OvHV-2)- Sheep associated malignant catarrhal fever virus of the genus Maca virus.
Epidemiology
- The Alcelaphine herpes virus-1 (AlHV-1) is maintained by inapparently infected wildebeest and transmits the disease to cattle in Africa and ruminant species (buffalo, deer and bison) in zoological garden.
- Ovine herpes virus-2 is prevalent in domestic sheep as a subclinical infection and causes MCF in cattle in most region of the world.
Source of infection
- The virus is excreted only in natural host of wildebeest and sheep respectively. These animals act as a source of infection for other animals.
- The virus is not excreted from clinically affected cattle. So, infected cattle will not be source of infection for another cattle.
Transmission
Wildebeest associated MCF Virus
- Inhalation of aerosol or ingestion of pasture contaminated by virus excreted in nasal and ocular discharge of young wildebeest.
- Infected young wildebeest have persistent viraemia for upto 3 months of age.
Sheep associated MCF Virus is spread by unknown means
- The epidemiological association of contact with lambing ewes suggest that perinatal lambs play a role in transmission similar to that of wildebeest calves. However, there is no evidence for transplcental transmission.
- Infection can also occur when cattle and sheep housed in the same building.
Clinical manifestation
- Incubation period is 3-8 weeks.
- The symptoms occur as peracute, alimentary tract form, head and eye form and mild form.
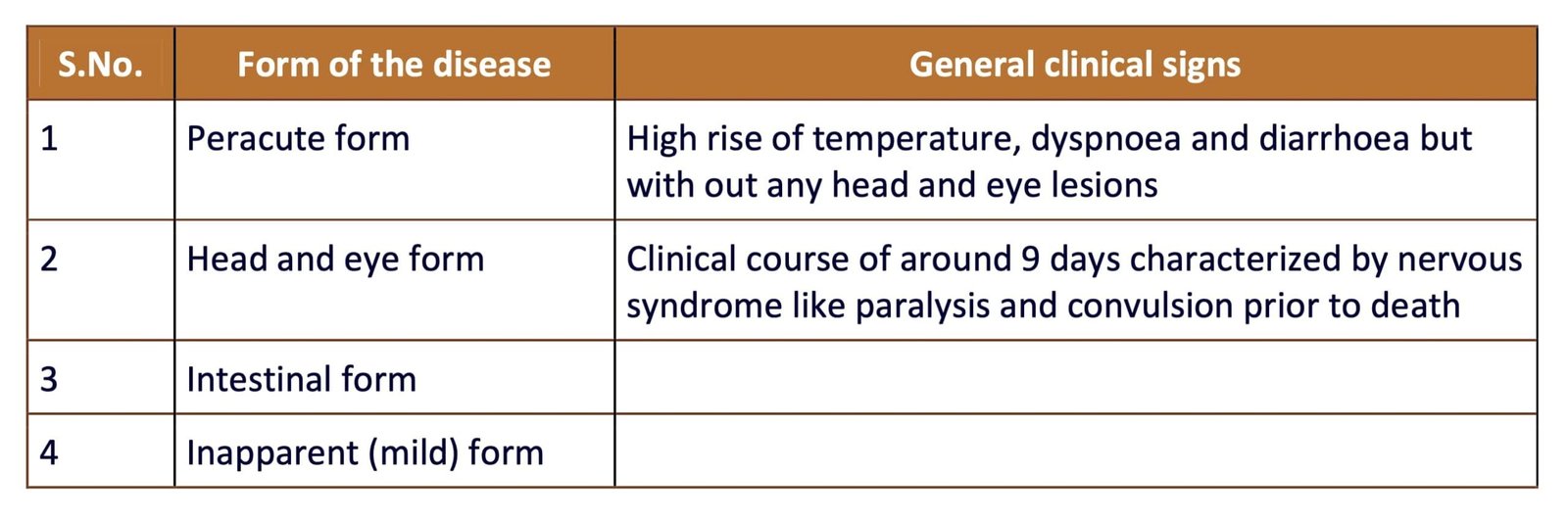
Peracute form
- Course of disease 1-3 days
- There is usually a high fever, dyspnea and acute gastroenteritis
Head and eye form (most common)
- Extreme dejection
- Anorexia
- Agalactia
- High fever (40-41.5o C)
- Rapid pulse rate (100-120/ min)
- Profuse mucopurulent nasal discharge
- Severe dyspnoea with stertor due to obstruction of nasal cavities with exudates
- Ocular discharge with oedema of the eyelids
- Blepharospasm
- Congestion of scleral vessels
- Superficial necrosis of anterior nasal and buccal mucosae
- Discrete local area of necrosis appear on the gum, hard palate, gingivae, dorsum of the tongue, commissures of mouth and inside the lips
- Cheek papillae is haemorrhagic especially at the tips
- Excessive ropy, bubbly salivation
- Necrosis of skin horn junction of feet especially at the back of the pastern
- Nervous signs- includes weakness in one leg, incoordination, demented appearance, muscle tremor, nystagmus, head pushing, paralysis and convulsions
- Lymphadenopathy
- Opacity of the cornea, commence as a narrow gray ring at the corneoscleral junction and hypopyon observed in some cases
- In some cases gross hematuria with red coloration is most marked at the end of urination
- Skin changes include local papule formation with clumping of hair into tufts over the loin and withers
- Persistence of the fever is a characteristic of MCF, even cases that persist for several weeks
Alimentary tract form
- The symptom resembles the head and eye form except marked diarrhoea and conjunctivitis
Inapparent (Mild) form
- Liver is swollen
- Haemorrhage in urinary bladder
- All lymph nodes are swollen and edematous and haemorrhagic
- Histopathology- necrotizing vasculitis with infiltration of lymphoblast like cells and macrophage in tunica media and tunica adventia is a pathognomic lesion of MCF
Sample Collection
- Buffy coat, Lymph node, spleen and lung
Diagnosis
- Based on clinical symptoms
- Based on necropsy finding
- Isolation of virus is difficult
- Identification of viral nucleic acid by PCR
- Competitive inhibition ELISA used for detection of antibodies in serum
- Nested PCR is commonly used for diagnosis
Differential Diagnosis
- Mucosal disease
- IBRT
- Rinderpest
- Sporadic bovine encephalomyelitis
- Theileriosis
Treatment
- There is no specific treatment; the anti-inflammatory drugs (NSAIDs) may ease the discomfort.
Control
- Housing of sheep and cattle in separate shed
- Avoid mixed grazing of cattle with sheep
- No vaccine is currently available
- Avoid grazing of cattle with wildebeest

