TABLE OF CONTENTS
Fracture of carpal bone
Fracture of carpal bone may be intra-articular or accessory carpal bone fracture in animals.
Intra articular fracture
Although most horses with intra-articular fracture of the carpus display acute onset of clinical signs, the damage is chronic in nature, at least in racehorses, and occurs at consistent sites in the dorsal aspect of the joints. The damage is the end result of a chronic process in which stressrelated subchondral bone damage occurs.53 Acute fracture and fragmentation of the carpus can occur, but this is typically in unusual locations, especially in the palmar aspect of the joints. Therefore, in equine athletes, and particularly racehorses, the damage occurs in predictable sites that lend themselves to more accurate prognosis with treatment.
Three types of fractures can occur within the carpal joints of the horse-
- Osteochondral fragmentation
- Slab fracture
- Comminuted fracture
Osteochondral fragmentation
Osteochondral fragmentation occurs on a single articular surface and is commonly found on the radial carpal, third carpal, intermediate carpal bones, and distal radius. The fragments can be attached with fibrous tissue, loose, or free within the joint, and are categorized as:
- recent and complete fragment,
- fragment with capsule attachment,
- chronic fragment with bone attachment, usually by fibrous tissue, or
- Fragment with extensive attachment to the bone.
Slab fracture
Slab fractures of the carpus usually occur completely through the bone, and although they are most common in the third carpal bone, they can occur in the intermediate and radial carpal bones as well. These fractures can also occur on the intermediate facet, both facets, or in a sagittal orientation.
Comminuted fractures
Comminuted fractures of the carpus occasionally occur, and although they primarily involve the third carpal bone, they can also involve the radial carpal, intermediate carpal, and fourth carpal bones. Horses that suffer these fractures are usually axially unstable. They require emergency stabilization and usually surgery to be sound for breeding.
Etiology
- Fatigue, increased speed, poor racing surface, poor trimming, possible uncoordinated movement and variability in racing surface.
- Subtle geometric abnormalities
- Chronic high load and instantaneous maximum load
- Soft tissue fatigue that can occur within the joints includes a decrease in soft tissue support of the joint capsule and the surrounding tendons and ligaments.
Clinical Signs
- Various degree of lameness
- Synovial effusion
- Soft tissue swelling
- Carpal flexion during standing
- Horses with small osteochondral carpal fragments experiencing subtle lameness, with mild amount of effusion and soft tissue swelling
- Characteristic of movement – abduction of forelimb with minimal carpal flexion, consequently this decreases hoof height during flight.
Diagnosis
- Radiographic examination – minimum of 6 radiographic views are needed. Both limbs should be radiographed
- Nuclear scintigraphy
- MRT
- CT
Treatment
- Arthroscopic removal of fragment
- Reduction of synovitis
- Degeneration of articular cartilage and bone have been graded for severity and correlated with outcome:
Grade 1: Minimal fibrillation or fragmentation at the edge of the defect left by the fragment, extending no more than 5 mm from the fracture line.
Grade 2: Articular cartilage degeneration extending more than 5 mm back from the defect and including up to 30% of the articular surface of that bone.
Grade 3: Loss of 50% or more of the articular cartilage from the affected carpal bone.
Grade 4: Significant loss of subchondral bone (usually distal radial carpal bone lesions).
- Slab fractures usually require internal fixation, such as lag screw fixation, to provide the best chance of achieving athletic soundness. However, thin slab fractures (less than 5 mm) can be removed because often they will not support lag screw repair.

Comminuted fractures require internal fixation or arthrodesis to restore axial stability to the limb and give the horse a chance to become pasture sound. The immediate stability gained from internal fixation improves the time to pain-free limb use and prevents overuse and consequent laminitis in the opposing limb.
Conservative therapy with casting and/or splints results in more prolonged lameness, which can lead to cast sores within the limb and often laminitis within the opposing limb. Conservatively treated horses sometimes heal with a deviation and significant chronic pain in the limb.
It is unusual for a horse to achieve athletic soundness after such an injury because the joint surface damage is often severe.
Lag screw fixation can be used to stabilize individual fractures; however, in severely comminuted injuries internal fixation with plates may be necessary and partial or full arthrodesis needed.
Post operative care
For osteochondral fragmentation, sutures are removed at 10 days and horses maintained in a bandage for 10 days. One common sequelae to carpal bandages is the creation of sores over the accessory carpal bone and the medial distal condyle of the radius. There are several ways to prevent these, including padding on either side of the structures, creating a window in the bandage for these areas to be exposed, or using super glue or adherent drapes over the incision sites without a bandage. Most clinicians prefer bandages because the compression helps decrease postoperative swelling; however, it has been observed that super glue has worked well.
The time needed for rehabilitation depends on the amount of damage, and the intensity of postoperative rehabilitation depends on the amount of articular cartilage damage and where the damage occurred. Rehabilitation is faster for the antebrachial carpal joint than the middle carpal joint because damage in the former is less common on the weight-bearing joint surface and consequently suffers minimal stress-induced damage. In general, most surgeons recommend 2 weeks of stall rest followed by 2 to 4 weeks of stall rest and hand walking, and then 2 to 4 additional weeks of turnout or swimming for problems within the antebrachial joint.
For mild to moderate damage within the middle carpal joint, the recommendation
is 2 to 4 weeks of stall rest, 4 weeks of stall rest and hand walking, and 8 weeks of turn-out or swimming; for severe middle carpal joint lesions or global articular cartilage damage, 4 to 6 months of rest are often recommended. Typically horses with slab fractures require 4 weeks of stall rest, 8 weeks of stall rest and hand walking, and 2 to 3 months of paddock turn-out. Horses should be radiographed prior to training, and rarely will the screw need to be removed.
In addition to rehabilitation, some form of intra-articular therapy is recommended to reduce inflammation and speed healing, especially of articular cartilage. If intra-articular medication is needed, the horses can be injected at the time of suture removal or after. Interleukin-1 receptor antagonist protein (IRAP) or polysulfated glycosaminoglycan/hyaluronic acid combination (with amikacin) once weekly for 3 weeks, starting 2 weeks after surgery. Treatment with IRAP is not uncommon, especially for severe joint damage, because the growth factor content within this product can be significant and theoretically help with articular cartilage healing. Intra-articular hyaluronic acid and polysulfated glycosaminoglycan are thought to promote healing and decrease inflammation.
Some surgeons find intra-articular stem cell therapy to be beneficial, although a study showed minimal benefit in experimental osteochondral fragmentation. Theoretically, the stem cells could promote release of growth factors into the joint, affecting on articular cartilage healing of a defect.
Some surgeons use systemic nonsteroidal anti-inflammatory medications for horses with carpal fractures, either phenylbutazone or Equioxx therapy. Local application of Surpass has also been shown to be beneficial both clinically and in experimental studies. Although systemic polysulfated glycosaminoglycan and intravenous hyaluronic acid therapies generally have shown modest effects, they may help maintain horses with carpal damage.
The use of passive range of motion and swimming if significant joint capsule damage is noted at the time of surgery. Potential postoperative problems include sepsis and subcutaneous infection. Problems such as persistent effusion and osteophyte formation are usually a result of the primary disease process, although excessive debridement of the joint capsule can lead to enthesiophyte formation.
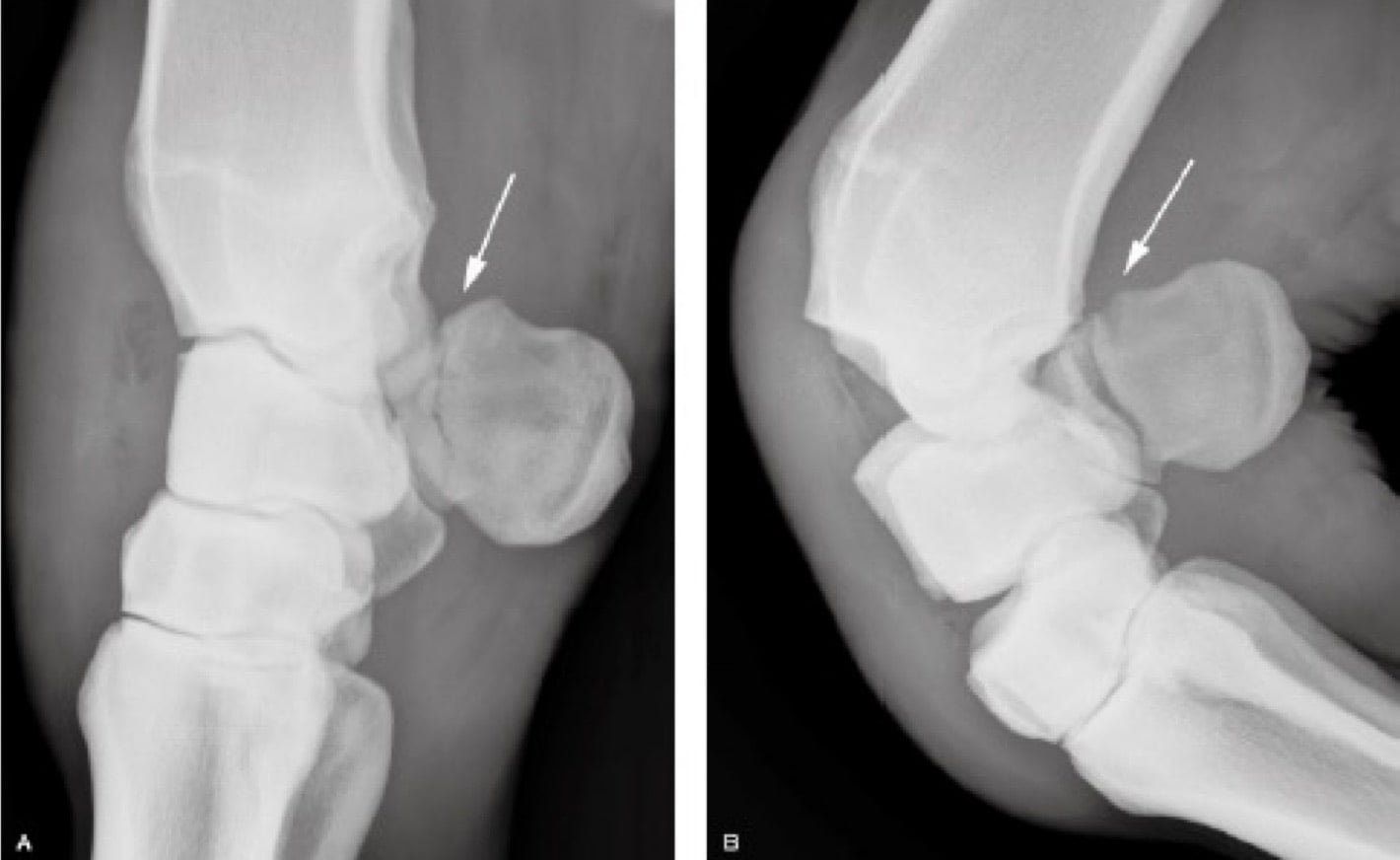
Accessory carpal bone fracture
Fracture of the accessory carpal bone can occur in any breed and primarily occurs in the frontal plane through the lateral groove of the bone. It is hypothesized that most of these fractures heal by fibrocartilaginous nonunion due to the constant pull from the flexor muscles.
Etiology
- External trauma
- Extreme internal forces such as asynchronous contraction of the flexor carpi ulnaris and ulnaris lateralis muscles
- Horses landing partially flexed, leading to a bowstring effect of the flexor carpi ulnaris lateralis and flexor tendons
Clinical signs and Diagnosis
- Horses with fractured accessory carpal bone typically have acute lameness with or without dorsal carpal or carpal canal swelling.
- There is often palpable pain over the accessory carpal bone, crepitus is sometimes felt, and sometimes with flexion, lateral to medial instability can be palpated.
- Care must be taken in examining these horses because they are very painful with flexion and may stand with their carpus flexed.
- One frequent clinical sign is a decrease in digital pulses with flexion.
- Radiographs are often sufficient; however, ultrasound examination of the carpal canal can help to characterize the extent of damage.
- Ultrasound examination should be repeated during the healing process because fibrous union is common, and expansion of this fibrous response could impinge the carpal canal, leading to pain.
- It is thought that severely comminuted fractures could increase the chance of carpal canal involvement.
Treatment and Prognosis
- Three to 6 months of rest or lag screw fixation are recommended.
- Ulnar neurectomy and arthroscopic surgery and debridement have also been recommended, but subtotal resection is no longer advocated.
- Small fragments involving the proximal dorsal aspect of the accessory carpal bone may involve the palmar aspect of the antebrachiocarpal joint and can be removed arthroscopically.
- However, because involvement of the carpal canal is often delayed until well into the healing phase, tenoscopic examination and retinacular release, if needed, also may be delayed.
- Periodic radiographs should follow treatment; distraction and further lysis of the fracture due to the fibrocartilaginous nonunion may be seen over time.
- Prognosis for healing is good. Although return to soundness is generally good, it can be reduced if significant carpal canal involvement is evident.