TABLE OF CONTENTS
Equine Influenza (Equine Distemper)
Equine Influenza (Equine Distemper) also known as Typhoid fever and pink eye disease.
Equine Influenza (Equine Distemper) is an acute highly viral disease of horses characterized by generalised septicaemia, respiratory problem accompanied by severe persistent dry cough.
Etiology
- Equine influenza is caused by influenza A / equine-1 (H7N7) or influenza A/equine- 2 (H3N8) virus is an Orthomyxovirus.
- There is no cross protection between subtypes.
- The entire outbreak in the past two decades has been caused by H3N8.
- The virus can travel upto 30 kms in an environment.
- Antigenic drift in the major surface protein hemagglutinin contributes to continuing susceptibility of horse to infection and reduced vaccine efficacy.
Epidemiology
- The disease is worldwide in distribution except Australia and Newzealand. In contrast, the H3N8 subtype isolated from horses in China was more closely related to avian strains.
- All age group of horse including newborn foals are susceptible. However, most cases of the disease occur in 2 years old or younger horse.
- Outbreak can occur at any time of the year.
Transmission
- Direct contact with an infected animals.
- Inhalation of aerosol discharged from an infected material.
- Fomite transfer on veterinary clothing and equipment.
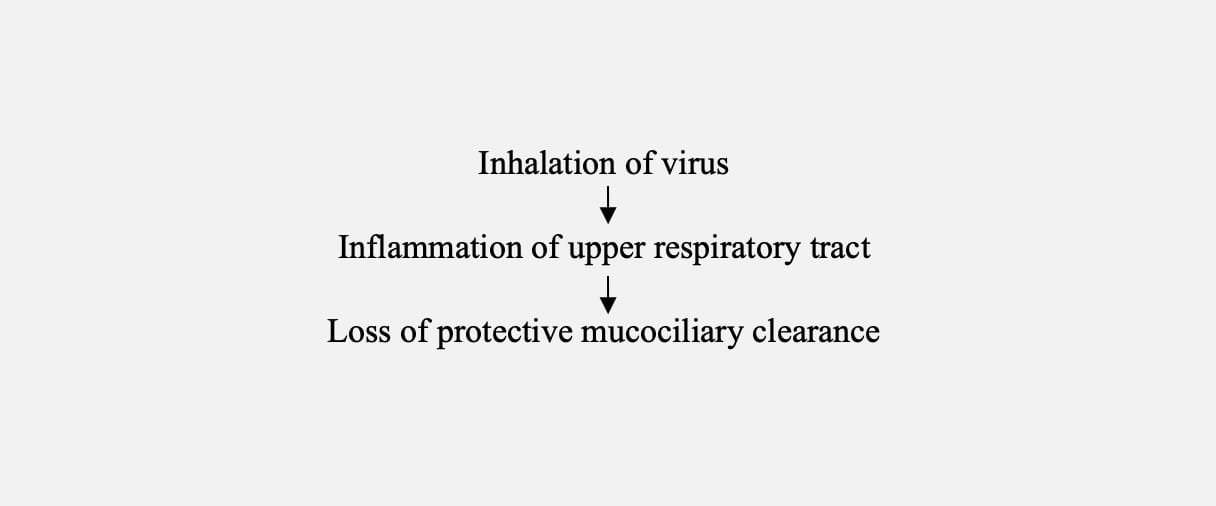
Pathogenesis
Clinical manifestation
- Incubation period- 2-3 days.
- Fever (101-106oF).
- Dry hacking cough in the beginning and moist cough later.
- During early stage of disease, nasal discharge is not prominenet sign, only mild watery discharge occur.
- Pain on palpation of submaxillary lymph node without marked swelling.
- Abnormal lung sound is characterized by crackles, wheezes and increased intensity of normal breath sound.
- The secondary bacterial complication causes severe bronchitis, pneumonia and edema of the legs. The animal shows depression, anorexia and reluctant to move.
Sample collection
- Live animals:
- Nasopharyngeal swab should be collected by inserting a sterile cotton swab approximately 30 cm into the nostril in the adult horse during rise of temperature.
- Paired sera sample.
Diagnosis
- Based on clinical signs.
- Isolation of virus in embryonated hens egg or cell culture.
- Detection of viral antigen by haemagglutination test (HA), Fluorescence antibody technique (FAT), ELISA and polymerase chain reaction (PCR).
- Detection of antibody titre in serum by haemagglutination inhibition test (HI) and single radial hemolysis test (SRH).
Treatment
- Antibitotics should be used to prevent secondary bacterial complications.
- Anti-inflammatory drugs should be used judiciously.
- Provide rest and dust free environment.
Prevention
- Several inactivated vaccines are commercially available.
- However, immunity is usually short-lived and booster injections are required in accordance with manufacturer’s instructions.
- Inactivated subunit vaccine containing immunogenic protein in an immune stimulating complex (ISCOM) induce a more sustained and greater immune response than conventional vaccine.
- Older horse should receive frequent booster before racing and show season.
- Mares should be revaccinated before being shipped to breeding farm.
- Foals should be vaccinated at 6 months of age and booster dose given at 21 days later and revaccination should be done every 6 months interval.
Control
- Avoid movement of horse between barn and paddock.
- Isolation of infected animal for 21 days.
- Cleaning, disinfection of infected premises.
- Vaccination of clinically normal horse during the face of the outbreak may enhance an immunity.

