TABLE OF CONTENTS
Aberrations of Estrus and Oestrous Cycle
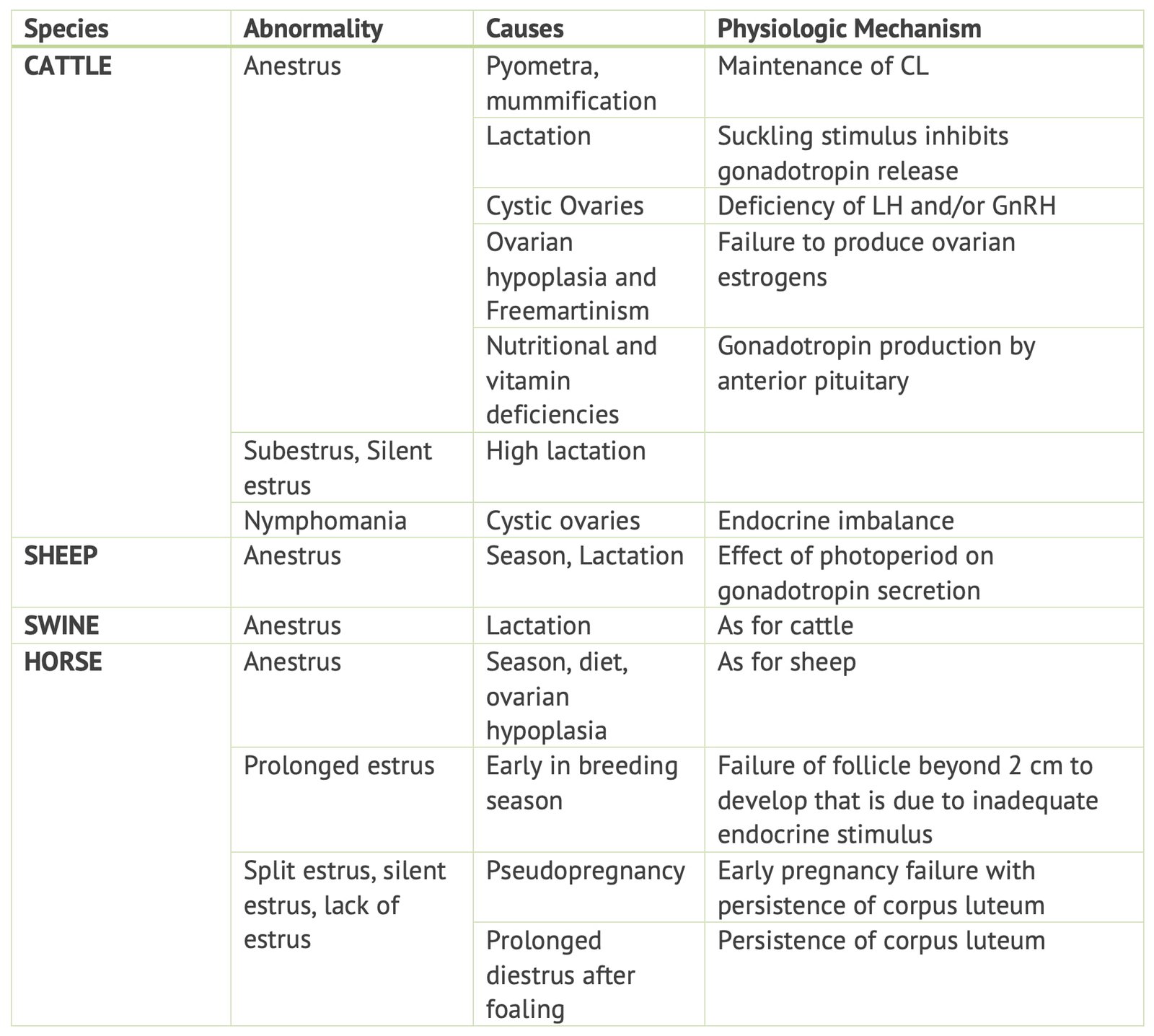
Aberrations of estrus and the oestrous cycle refer to deviations from the normal reproductive cycle in female animals, often caused by hormonal imbalances, genetic factors, nutritional deficiencies, or environmental stressors.
Aberrations of estrus and the oestrous cycle can manifest as anestrus (absence of estrus), prolonged estrus, silent heat (estrus without visible signs), irregular cycle lengths, or cystic ovarian conditions.

Aberrations of Estrus and Oestrous Cycle in Cows
Sub estrous / Silent heat / Quiet ovulators
Ovulations occur without behavioural manifestation of estrus. The first and second ovulation postpartum are often not proceed by behavioural signs of estrus and are thus are truly ‘Silent heats’.
In heifers, the estrus associated with first ovulation is usually silent.
Causes of Silent heat
A sub threshold of hormone production or an imbalance between hormones.
Nutritional defficiencies such as defficiency of ß Carotene, Phosphorous, Copper, Cobalt etc.
Diagnosis of Silent heat
- Clinical history
- Rectal palpation of the genital system
Treatment of Silent heat
If a mature Cl is present, PGF2α or an analogue followed by Timed Artificial Insemination (TAI) can be carried out. If a CL is at refractory stage, double injection PG regimen at 11 days interval could be used.
Alternatively PRID or other progesterone implants could be used followed by fixed time insemination.
Anoestrum
Failure of estrum or anestrum is the principle symptom of many conditions that may affect the estrous cycle. Anestrum is observed most commonly either:
- After parturition as post partum or Pre service anestrum.
- Following service-Post service anestrum (when conception does not occur).
It is due to multiple causes and often not directly related to endocrine system.
Diagnosis is based on:
- history
- careful clinical examination of the genital tract and ovaries per rectum and vagina by a speculum.
- physical examination of the cow for accurate differential diagnosis.
Delayed Ovulation
If ovulation occurs more than 18 hrs after the end of heat, then ovulation is said to be delayed.
Delayed Ovulation caused by:
- Endocrine defficiency or imbalance
- Failure of development of hormone receptors at the target tissue
- Mechanical factors
Delayed ovulation is generally assumed to be one of the causes for failure of conception in Repeat Breeders and is diagnosed by palpation of mature follicle on the ovary more than 24-48 hours after the end of estrum.
Aberrations of Estrus and Oestrous Cycle in Mares
Irregularities of Oestrous Cycle
Irregularities of the estrous cycle in mares may be associated with:
- Ovarian pathology
- Uterine pathology
- Apparent functional abnormalities of the ovarian hypophyseal axis.
Abnormalities of endocrinology, cyclicity, or ovulation are uncommon in mares with normal reproductive tracts, and hence, other causes of infertility should be ruled out before abnormal cyclicity is implicated as a cause of infertility.
Cystic ovaries, as seen in cattle, do not occur in mares.
Apparent estrous cycle irregularities that are not associated with pathology include:
- prolonged anovulatory estrus during the transition period,
- “silent heat”,
- prolonged luteal activity,
- estrus during pregnancy,
- “persistent estrus” or behavioural changes attributable to estrus.
Diagnosis of the cause of estrous cycle irregularities in mares is based on:
- History
- Teasing records
- Findings on palpation
- Ultrasonography
- Determination of hormone concentrations
Assessment of Oestrous Cycle and Ovulation
An important factor to remember when evaluating apparent cycle abnormalities is the normal variation in length of estrus.
- The normal estrous cycle length ranges from 2 to 12 days.
- The length of cycle is generally repeatable within mares, but is longer at the beginning and end of the breeding season.
Teasing is a major determinant of apparent cyclicity.
- Individual teasing with an active stallion is the best method of heat detection.
- Should be performed at least three times weekly. The mare‘s behavior should be scored by a knowledgeable individual.
- “Silent heat” may occur in normally cyclic mares.
Knowledge of the estrus and diestrus reactions of each individual mare is crucial; a mare in heat may be less demonstrative than another mare in diestrus.
- Some mares may show signs of estrus immediately on contact with the stallion.
- Some mares may require teasing for 3 to 4 minutes before they respond.
A mare that shows no change in behaviour at all during her cycle should be examined regularly by transrectal palpation and ultrasonography to detect estrus.
Estrus behaviour can also be seen in mares:
- During seasonal anestrus
- In mares that have been ovariectomized
- In mares with gonadal dysgenesis
The length of diestrus is more repeatable among mares than is the length of estrus, at 15-20 days.
A pattern of high progesterone for about 15 days followed by low progesterone four more days is strongly indicative of normal cyclicity.
Ovarian and Uterine Characteristics of Normal Cyclicity
In assessing the normality of follicle growth and ovulation, the large variation in follicle size at ovulation should be recognized.
- The size of follicles at ovulation is commonly 35 to 45 mm diameter, but mares can ovulate much smaller follicles or larger follicles, with normal fertility.
- Follicle size at ovulation is often repeatable for a given mare.
- Follicle size at ovulation also decreases toward the middle of the breeding season.
- Numerous large follicles and corpora lutea are normally present on the ovaries of pregnant mares, especially between 30 and 120 days. These are sometimes mistaken for ovarian pathology.
Transrectal palpation and ultrasonography are indispensable tools in the evaluation of the estrous cycle.
Uterine changes detectable on ultrasonographic examination are also helpful in estimating the stage of the estrous cycle in mares with questionable estrus behavior.
Physiological Estrus Irregularity
The Transitional Period
- The mare is a seasonal, long-day breeder
- Mares enter anestrus during the winter months.
- The period between late anestrus and the first ovulation of the year is termed the transitional period.
- Follicular growth occurs due to sufficient Pituitary gonadotropin output but normal follicle maturation and ovulation do not take place.
- Palpation and Ultrasonography may not be helpful in distinguishing from normal follicles; however, they may be structurally and hormonally abnormal.
- During the transitional period, mares may exhibit constant or irregular estrus, as a response to rising and falling estrogen from waves of non ovulatory follicles.
- When estrus behavior does subside, it may recur within days; there is no normal diestrus interval.
- Diagnosis is based on the season of the year, lack of evidence of ovulation and multiple small to large follicles present on both ovaries.
Cycle Irregularities Associated with Aging
- Mares cycle less efficiently after about 20 years of age.
- Cycles may cease over 25 years.
- These mares may be presented because of erratic or constant heat during the breeding season, or because multiple breeding have not resulted in pregnancy. They may also be apparently anestrus during the breeding season.
- Diagnosis is based on the mare‘s age; these changes are not usually seen until the mare is near 20 years of age.
- Breedings during this time will not result in pregnancy because the mare does not ovulate
- Treatment with pulsatile gonadotrophin- releasing hormone may be effective in inducing follicular growth and ovulation.
- Mares over 25 years of age may cease cycling altogether. These mares may be presented because of erratic or constant heat during the breeding season, or because multiple breeding have not resulted in pregnancy. They may also be apparently anestrus during the breeding season.
Fertility is reduced due to:
- Decreased oocyte viability and uterine changes
- Longer follicular phase
- Fewer ovulations per year
Prolonged Luteal Activity
A prolonged luteal phase is common in mares:
- Normally occurs in 4 to 18 percent of cycles
- Severe damage to the endometrium, as seen in cases of pyometra. If the damage is severe enough that prostaglandin production is impaired, retention of the primary CL results.
Differential diagnosis includes:
- Pregnancy
- Silent heat
- Poor estrus detection
- Short heats that are missed, especially near the middle of the breeding season
Diagnosis is based on finding a normal non-pregnant diestrus reproductive tract associated with failure to show estrus or failure during examination and to find changes consistent with estrus for more than 2 weeks after ovulation. Progesterone concentrations will be high for more than 2 weeks.
Treatment involves administration of prostaglandin F2α. To assure a response, the prostaglandin should be given at least 5 days after the most recent ovulation. Return to heat occurs in about 3 days.
Shortened Luteal Phase
A decrease in the length of diestrus may be indicative of premature luteolysis.
Shortened Luteal Phase may be associated with:
- Endometritis
- Prostaglandin production associated with uterine inflammation or bacterial endotoxin production
- May be both
If a shortened luteal phase is detected, an endometrial culture and biopsy should be obtained to determine if endometritis is present, and, if so, which organism may be responsible.
Resolution of endometritis should result in return of normal diestrus intervals.
Persistant Estrus
- “Persistent estrus” is a fairly common complaint in working and racing mares.
- When evaluating cases of persistent estrus, the normal variation of estrus length, from 2 to over 10 days, should be considered.
- A major confusing issue in these mares is what is considered to be estrus behavior. Such mares may be characterized by their owner as being irritable, kicking when their sides are touched, leaning on the handler, striking, urinating, or wringing their tails interpreted as heat; however, they may be simply signs of agitation.
- To diagnose the cause of the apparent estrus behavior, findings on palpation and ultrasonography of the reproductive tract are evaluated along with the history, and the mare should be teased with an active stallion.
- Mares with large follicles may respond to administration of human chorionic gonadotrophin by ovulating approximately 2 days late and going out of heat in another 1 to 2 days.
- Mares that have constant agitated behavior, rather than true estrous behavior, may be in any stage of the estrous cycle at the time of examination. When evaluated critically, although some signs associated with estrus may be present the behavior of the agitated mare is anxious or guarding. She is resentful of the approach of a stallion when teased and may lean away from the stallion or appear fearful. This is in contrast to the mare in true estrus who; during teasing, is typically calm, submissive, and interested in maintaining contact with the stallion.
- Abnormal estrus-type or aggressive behavior may be associated with granulose cell or other ovarian tumors.
- Signs of persistent estrus may be attributable to vaginal inflammation due to aspiration of air into the vagina when the mare is working. These mares lack perineal fat, which affects tone of the vulvar lips, the angle of the vulva, and the weight of the perineal body.
- The mare has signs of vaginitis such as frequent urination, hunching the back, dragging the hind feet, and wringing the tail. Racing mares commonly have a history of “stopping” or “pulling up” part way through training periods; this may be due to pneumovagina incurred during work.
- Examination of the tract shows the mare at any stage of the cycle; bright echogenic particles representing air may be seen in the vagina or uterus or both during ultrasonographic examination.
- Vaginoscopy may reveal inflammation and the mare may show extreme signs of irritation after the speculum is inserted or removed. This problem may occur even after Caslick‘s surgery has been performed.
- Abnormalities of the bladder or urethra, such as cystitis or urethral masses, may result in frequent urination that is interpreted as persistent estrus.
Cyclic Behavioural Problems Associated with Oestrus
Some mares become hard to manage, perform irregularly, or even appear lame when in heat; this behavior is intermittent and corresponds to specific stage of the estrous cycle.
Altrenogest is commonly used to suppress problem estrus behaviour in mares and may be effective.
Ovariectomies for mares should be reserved only for cases in which the mare has cyclic behavioural problems corresponding to a specific part of the estrous cycle; this behaviour should seem to improve over the winter.
Occasionally a mare is presented that has vicious outbursts of aggressive behavior. Such mares should be approached with caution. Little information is available on the cause of this behaviour but it is unlikely to be related to the reproductive tract.
Cyclic Irregularities Associated with Ovarian Pathology
Gonadal Dysgenesis
- Gonadal dysgenesis refers to congenital lack of development of the ovaries.
- Only a “streak” gonad is present, with no follicular activity. The remainder of the tract is intact but juvenile because no ovarian steroids are present to induce secondary development.
- Condition is most commonly associated with defects of the X chromosome, including XO and XXX; however. It may be seen in mares with apparently normal karyotypes.
- Presenting signs include anestrus, erratic estrus, or constant estrus. Exhibition of estrus behavior is due to lack of progesterone.
- Diagnosis of gonadal dysgenesis is based on history, karyotype and repeated palpation and ultrasonography or progesterone determination. Mares with gonadal dysgenesis have never foaled and have never been pregnant. Palpation and ultrasonography reveal very small or apparently absent ovaries; if ovaries are present, no follicular activity is seen.
- A chromosomal abnormality on karyotype supports the diagnosis of gonadal dysgenesis. No treatment is possible for these mares.
Anovulation or failure of ovulation
Failure of ovulation is often preceded by an anovulatory estrus, with follicle regressing and become atretic. Sometimes however a follicle does not regress, but having reached its maximum size of 2.0-2.5 cm in diameter the walls become luteinized. This structure behaves the same way as CL either regressing after 17-18 days or frequently much earlier so that the cow returns to estrus at a shorter than normal interval.
Diagnosis of anovulation can only be made retrospectively by noting on rectal palpation that a follicle persists longer than one would have suspected. In cases of lutenized follicle, it will remain for 17-19 days before regressing, the ovary containing it will be rounded, smooth, fluctuating rather than irregular and solid as it is with a CL.
Treatment is directed towards ensuring that ovulation occurs at the next estrus. Hence, hCG or GnRH is given. If ovarobursal adhesions are present, there is no treatment.